
Central diabetes insipidus:
A rare endocrine condition1-3
Clinical overview and terminology

~ 13,700
people in the US have CDI*
Central diabetes insipidus (CDI, now also known as AVP-D), is an endocrine condition characterized by insufficient levels of the antidiuretic hormone arginine vasopressin (AVP).4
CDI is a rare disease, affecting ~1 in 25,000 people worldwide1
This equates to ~13,700 patients in the United States.2*
- It occurs across all age groups, with presentation determined largely by etiology5
- The term AVP-D refers only to CDI, and does not cover nephrogenic diabetes insipidus (NDI; also known as arginine vasopressin resistance [AVP-R])4
- Using the term AVP-D instead of CDI helps prevent confusion with diabetes mellitus4
Based on an estimated United States population of 343,000,000 individuals.2
Differentiating CDI from NDI and primary polydipsia
CDI is a polyuria–polydipsia syndrome. These syndromes share overlapping symptoms but stem from very different mechanisms. Correctly distinguishing among these conditions is essential, as treatment approaches vary significantly.5
There are 3 main types of polyuria-polydipsia syndromes:

Central diabetes insipidus (CDI)
The most common form, caused by insufficient production or release of AVP from the pituitary gland5
Nephrogenic diabetes insipidus (NDI)

Primary polydipsia
A psychiatric condition involving excessive intake of large amounts of water despite normal AVP secretion and action5
Core characteristics of CDI
CDI is a rare polyuria-polydipsia syndrome characterized by inadequate secretion of arginine vasopressin (AVP) from the pituitary gland, resulting in:

Impaired renal water absorption5

Hypotonic polyuria (~2 to ~4 gallons of urine per day)6

Compensatory thirst/polydipsia (up to ~5 gallons of fluid per day)6

Etiologies
Understanding the underlying causes and pathophysiology of CDI contributes to accurate diagnosis and effective management.1

of CDI cases are idiopathic. When the cause is known, many cases are due to acquired or inherited damage to the posterior pituitary gland5,7


Based on a series of 79 patients with CDI seen at 4 pediatric endocrinology units between 1970 and 1996.8
Etiologies of acquired CDI5,7
- Trauma (surgery and deceleration injury)
- Neoplasia (craniopharyngioma, meningioma, germinoma and metastases)
- Vascular disorders (cerebral or hypothalamic hemorrhage and infarction or ligation of anterior communicating artery aneurysm)
- Granulomatous disorders (Langerhans cell histiocytosis and sarcoidosis)
- Infections (meningitis, encephalitis and tuberculosis)
- Inflammatory or autoimmune diseases (lymphocytic infundibuloneurohypophysitis and IgG4 neurohypophysitis)
- Drug or toxin exposure
- Osmoreceptor dysfunction
- Other (hydrocephalus, ventricular or suprasellar cyst, and degenerative diseases)
More than 1 in 3 cases of acquired CDI are due to head trauma or transfrontal/transsphenoidal surgery
Etiologies of inherited CDI5,9
- Autosomal dominant: AVP mutations
- Autosomal recessive, type a and b: AVP mutations
- Autosomal recessive, type c: WFS1‡ mutations
- Autosomal recessive, type d: PCSK1§ mutations
- X-linked recessive: gene unknown
- Septo-optic dysplasia
‡Wolfram syndrome-1.
§Proprotein convertase subtilisin/kexin type 1.
AVP signaling in healthy physiology and the pathophysiology of CDI
Overview of renal AVP function in healthy individuals1,5,10
Pathophysiological changes in CDI1,5,10


CDI is characterized by inadequate synthesis and/or secretion of AVP in response to osmotic stimulation
CDI induces water diuresis due to an inability to maximally concentrate urine


Upon detecting increased serum osmolality, the hypothalamus signals from the supraoptic and paraventricular nuclei to the posterior pituitary via magnocellular neurons to release AVP
When AVP binds to V2 receptors in the DCTs of the kidneys, aquaporin-2 channels translocate from the cytoplasm into the apical membrane of the DCT, allowing water to return to the circulation
Recognizing the signs, symptoms, and complications of untreated CDI
Early recognition of CDI is essential, as impaired water conservation can lead to progressive dehydration, electrolyte abnormalities, and systemic instability.5 Identifying symptom patterns promptly can help mitigate complications associated with untreated CDI.
Secondary symptoms and complications6,11



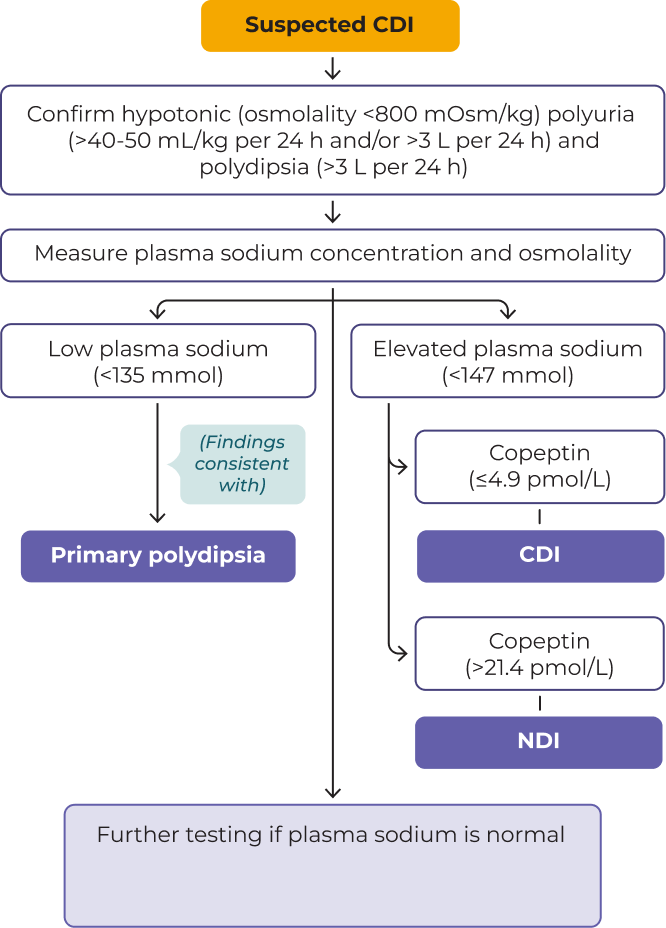
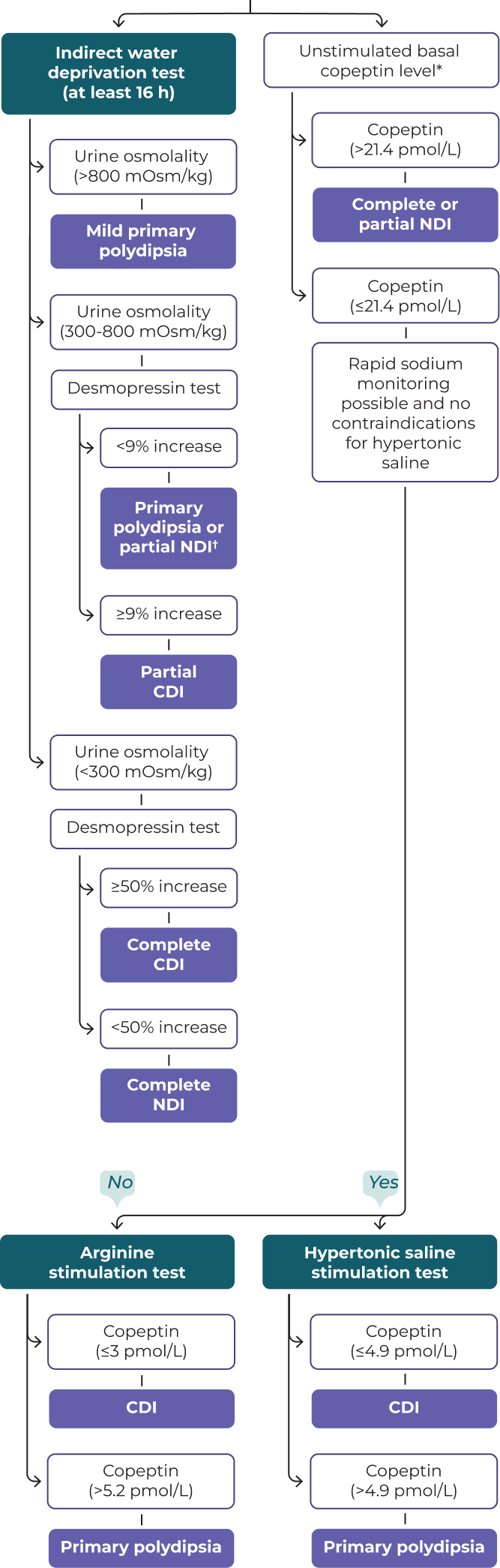
Diagnosing CDI: A structured approach to evaluation1
The diagnostic algorithm for CDI centers on 2 key decision points:
- In patients with polyuria-polydipsia syndrome, plasma sodium concentration and osmolality are measured
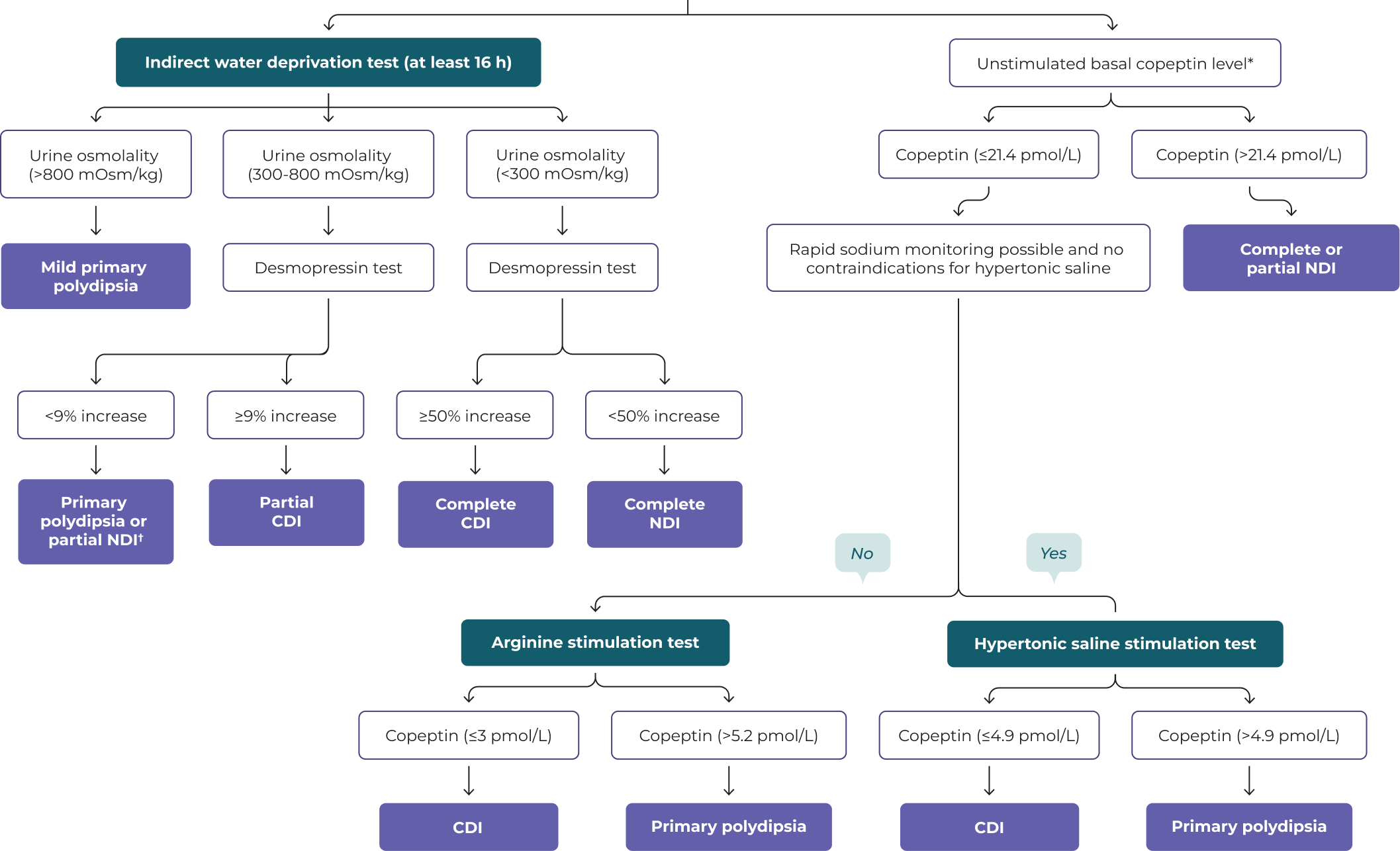
- If plasma sodium concentration and osmolality are in the normal range, further assessments are performed using either the indirect water deprivation test or copeptin-based testing
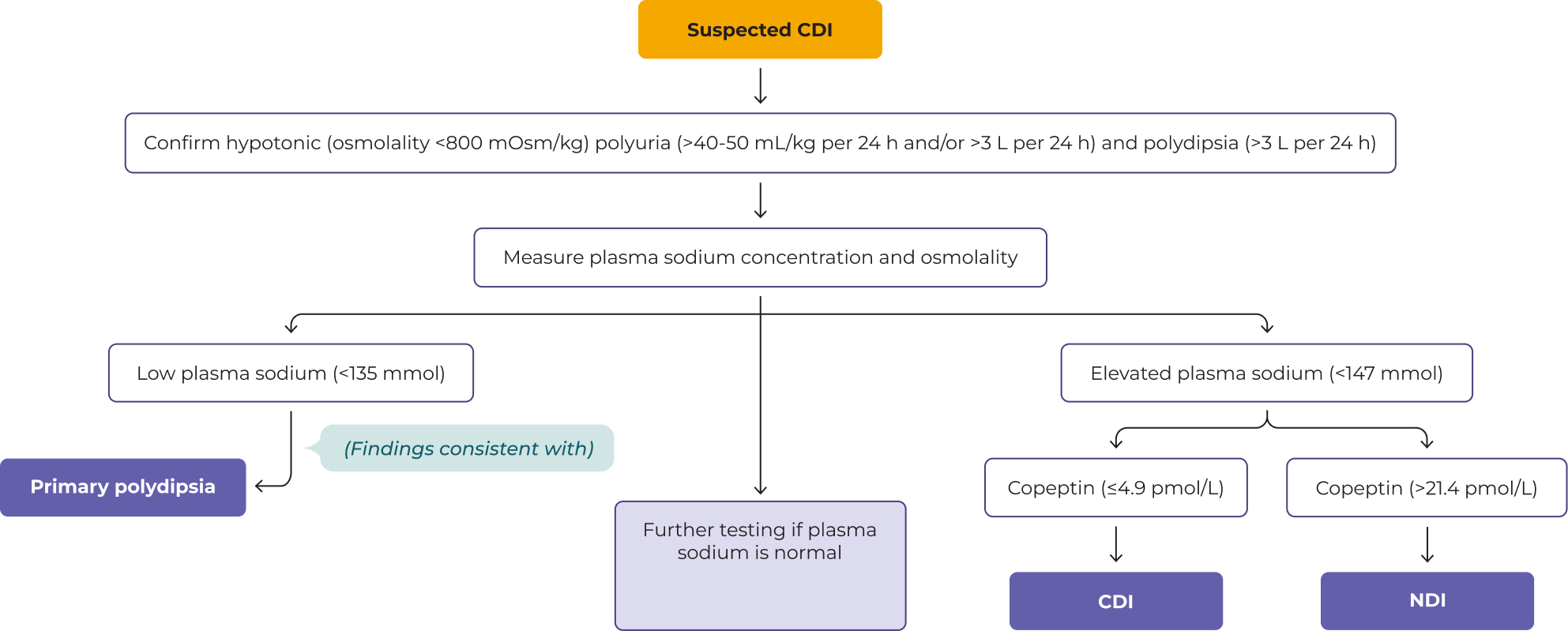
Adapted from: Atila C, Refardt J, Christ-Crain M. Arginine vasopressin deficiency: diagnosis, management and the relevance of oxytocin deficiency. Nat Rev Endocrinol. 2024;20(8):487-500.
Basal copeptin can only be validly evaluated if the patients had no distress (including physical and psychological) and had no severe nausea.
Adapted from: Atila C, Refardt J, Christ-Crain M. Arginine vasopressin deficiency: diagnosis, management and the relevance of oxytocin deficiency. Nat Rev Endocrinol. 2024;20(8):487-500.
Basal copeptin can only be validly evaluated if the patients had no distress (including physical and psychological) and had no severe nausea.
Plasma osmolality measurement might be needed to differentiate between both entities.
Learn how DESMODA helps bring precision, control, and flexibility to CDI management for patients of all ages12-18
References: 1. Atila C, Refardt J, Christ-Crain M. Arginine vasopressin deficiency: diagnosis, management and the relevance of oxytocin deficiency. Nat Rev Endocrinol. 2024;20(8):487-500. 2. World Health Organization. Health data overview for the United States of America. May 15, 2024. Accessed February 2, 2026. https://data.who.int/countries/840 3. U.S. Food & Drug Administration. Rare diseases at FDA. November 21, 2024. Accessed February 2, 2026. https://www.fda.gov/patients/rare-diseases-fda 4. Arima H, Cheetham T, Christ-Crain M, et al. Changing the name of diabetes insipidus: a position statement of the Working Group for Renaming Diabetes Insipidus. J Clin Endocrinol Metab. 2022;108(1):1-3. 5. Christ-Crain M, Bichet DG, Fenske WK, et al. Diabetes insipidus. Nat Rev Dis Primers. 2019;5(1):54. 6. Kalra S, Zargar AH, Jain SM, et al. Diabetes insipidus: the other diabetes. Indian J Endocrinol Metab. 2016;20(1):9-21. 7. Flynn K, Hatfield J, Brown K, Vietor N, Hoang T. Central and nephrogenic diabetes insipidus: updates on diagnosis and management. Front Endocrinol (Lausanne). 2025;15:1479764. 8. Maghnie M, Cosi G, Genovese E, et al. Central diabetes insipidus in children and young adults. N Engl J Med. 2000;343(14):998-1007. 9. Hetman M, Fułek M, Zajączkowska K, Żarczyńska A, Łagosz P, Barg E. The central diabetes insipidus associated with septo-optic dysplasia (de Morsier syndrome). Pediatr Endocrinol Diabetes Metab. 2018;24(4):197-203. 10. Mutter CM, Smith T, Menze O, Zakharia M, Nguyen H. Diabetes insipidus: pathogenesis, diagnosis, and clinical management. Cureus. 2021;13(2):e13523. 11. Yun G, Baek SH, Kim S. Evaluation and management of hypernatremia in adults: clinical perspectives. Korean J Intern Med. 2023;38(3):290-302. 12. DESMODA. Package Insert. Eton Pharmaceuticals, 2026. 13. Verrue C, Mehuys E, Bousery K, Remon JP, Petrovic M. Tablet-splitting: a common yet not so innocent practice. J Adv Nurs. 2011;67(1):26-32. 14. Chin X, Teo SW, Lim ST, Ng YH, Han HC, Yap F. Desmopressin therapy in children and adults: pharmacological considerations and clinical implications. Eur J Clin Pharmacol. 2022;78(6):907-917. 15. Gudeman J, Jozwiakowski M, Chollet J, Randell M. Potential risks of pharmacy compounding. Drugs R D. 2013;13(1):1-8. 16. Zhi L, Liu D, Shameem M. Injection site reactions of biologics and mitigation strategies. AAPS Open. 2025;11:5. 17. McLenon J, Rogers MAM. The fear of needles: A systematic review and meta-analysis. J Adv Nurs. 2019;75(1):30-42. 18. Centers for Disease Control and Prevention. Before, during, and after shots. CDC. August 9, 2024. Accessed February 2, 2026. https://www.cdc.gov/vaccines-children/before-during-after-shots/index.html
USE AND IMPORTANT SAFETY INFORMATION
INDICATION
DESMODA (desmopressin acetate) is a vasopressin analog indicated for the management of central diabetes insipidus as antidiuretic replacement therapy for adults and pediatric patients.
Limitations of Use
Do not use DESMODA for the treatment of nephrogenic diabetes insipidus.
IMPORTANT SAFETY INFORMATION
Contraindications
DESMODA is contraindicated in patients with hypersensitivity to desmopressin acetate or to any of the components of DESMODA, patients with moderate to severe renal impairment (adults with creatinine clearance (CLcr) less than 50 mL/min), or patients with hyponatremia or a history of hyponatremia.
Warnings and Precautions
Hyponatremia: Excessive fluid intake when urine output is limited by the antidiuretic effect of desmopressin may lead to water intoxication with hyponatremia. Cases of hyponatremia have been reported from postmarketing experience with desmopressin acetate. Monitor patients for signs or symptoms associated with hyponatremia, including headache, nausea/vomiting, weight gain, restlessness, fatigue, lethargy, confusion, depressed reflexes, muscle cramps or spasms, and abnormal mental status. Severe hyponatremia may result in seizures, coma, respiratory arrest, or death.
Fluid restriction is recommended during treatment and is particularly important in pediatric and geriatric patients, who are at increased risk. More frequent monitoring of serum sodium is recommended in patients with conditions associated with fluid and electrolyte imbalance or those receiving concomitant medications that may cause hyponatremia. Temporarily stop treatment with DESMODA during acute intercurrent illness characterized by fluid and/or electrolyte imbalance or under conditions associated with increased water intake.
Fluid Retention: Desmopressin acetate may cause fluid retention and should be used with caution in patients with heart failure or uncontrolled hypertension. DESMODA is not recommended in patients at risk for increased intracranial pressure or those with a history of urinary retention.
Hypersensitivity Reactions: Hypersensitivity reactions including anaphylaxis have been reported rarely with intravenous and nasal administration of desmopressin acetate. DESMODA is contraindicated in patients with known hypersensitivity to desmopressin acetate or any of the components of DESMODA.
Risk of Benzyl Alcohol Toxicity in Neonates: Serious adverse reactions, including fatal reactions, have been reported in low-birth-weight neonates and preterm neonates who received benzyl alcohol containing drugs intravenously. DESMODA contains benzoic acid, a metabolite of benzyl alcohol; the relationship between systemic benzoic acid exposure and toxicity is not well characterized. Use DESMODA with caution in low-birth-weight neonates or preterm neonates and monitor for signs and symptoms of metabolic acidosis.
Adverse Reactions
The serious adverse reactions associated with DESMODA are hyponatremia, fluid retention, hypersensitivity, and the risk of benzyl alcohol toxicity in neonates. Other common adverse reactions reported with desmopressin acetate include abnormal thinking, diarrhea, and edema/weight gain. Additional adverse reactions reported in clinical studies or postmarketing experience include nausea, vomiting, headache, fatigue, dizziness, water intoxication, seizures, confusion, hallucinations, urinary retention, and rash.
To report a suspected adverse event related to DESMODA, contact Eton Pharmaceuticals, Inc. at 1-855-224-0233 or the U.S. Food and Drug Administration (FDA) at https://www.fda.gov/safety/medwatch or call 1-800-FDA-1088.
Please see full Prescribing Information for more information.
USE AND IMPORTANT SAFETY INFORMATION
INDICATION
DESMODA (desmopressin acetate) is a vasopressin analog indicated for the management of central diabetes insipidus as antidiuretic replacement therapy for adults and pediatric patients.
Limitations of Use
Do not use DESMODA for the treatment of nephrogenic diabetes insipidus.
IMPORTANT SAFETY INFORMATION
Contraindications
DESMODA is contraindicated in patients with hypersensitivity to desmopressin acetate or to any of the components of DESMODA, patients with moderate to severe renal impairment (adults with creatinine clearance (CLcr) less than 50 mL/min), or patients with hyponatremia or a history of hyponatremia.
Warnings and Precautions
Hyponatremia: Excessive fluid intake when urine output is limited by the antidiuretic effect of desmopressin may lead to water intoxication with hyponatremia. Cases of hyponatremia have been reported from postmarketing experience with desmopressin acetate. Monitor patients for signs or symptoms associated with hyponatremia, including headache, nausea/vomiting, weight gain, restlessness, fatigue, lethargy, confusion, depressed reflexes, muscle cramps or spasms, and abnormal mental status. Severe hyponatremia may result in seizures, coma, respiratory arrest, or death.
Fluid restriction is recommended during treatment and is particularly important in pediatric and geriatric patients, who are at increased risk. More frequent monitoring of serum sodium is recommended in patients with conditions associated with fluid and electrolyte imbalance or those receiving concomitant medications that may cause hyponatremia. Temporarily stop treatment with DESMODA during acute intercurrent illness characterized by fluid and/or electrolyte imbalance or under conditions associated with increased water intake.
Fluid Retention: Desmopressin acetate may cause fluid retention and should be used with caution in patients with heart failure or uncontrolled hypertension. DESMODA is not recommended in patients at risk for increased intracranial pressure or those with a history of urinary retention.
Hypersensitivity Reactions: Hypersensitivity reactions including anaphylaxis have been reported rarely with intravenous and nasal administration of desmopressin acetate. DESMODA is contraindicated in patients with known hypersensitivity to desmopressin acetate or any of the components of DESMODA.
Risk of Benzyl Alcohol Toxicity in Neonates: Serious adverse reactions, including fatal reactions, have been reported in low-birth-weight neonates and preterm neonates who received benzyl alcohol containing drugs intravenously. DESMODA contains benzoic acid, a metabolite of benzyl alcohol; the relationship between systemic benzoic acid exposure and toxicity is not well characterized. Use DESMODA with caution in low-birth-weight neonates or preterm neonates and monitor for signs and symptoms of metabolic acidosis.
Adverse Reactions
The serious adverse reactions associated with DESMODA are hyponatremia, fluid retention, hypersensitivity, and the risk of benzyl alcohol toxicity in neonates. Other common adverse reactions reported with desmopressin acetate include abnormal thinking, diarrhea, and edema/weight gain. Additional adverse reactions reported in clinical studies or postmarketing experience include nausea, vomiting, headache, fatigue, dizziness, water intoxication, seizures, confusion, hallucinations, urinary retention, and rash.
To report a suspected adverse event related to DESMODA, contact Eton Pharmaceuticals, Inc. at 1-855-224-0233 or the U.S. Food and Drug Administration (FDA) at https://www.fda.gov/safety/medwatch or call 1-800-FDA-1088.
Please see full Prescribing Information for more information.